ここから本文です
日本における認知症予防の可能性-認知症の約4割は「予防」可能- ~主要因子は「難聴」、次いで「運動不足」。危険因子10%の低減で20万人の発症抑制へ~(Potential for Dementia Prevention in Japan - Nearly 40% of Dementia Cases Are Preventable - ~Hearing Loss Identified as the Leading Risk Factor, Followed by Physical Inactivity~)

2026年01月13日
東海大学[伊勢原キャンパス]医学部の和佐野浩一郎教授およびデンマーク・コペンハーゲン大学認知症センターのカスパー・ヨーゲンセン上席研究員による国際共同研究グループは、日本の公的統計や疫学データを用いた解析により、国内の認知症の38.9%が生活習慣や健康状態の改善によって、理論的には予防可能であることを明らかにしました。
本研究では、日本における最大の危険因子が「難聴(6.7%)」であり、次いで「運動不足(6.0%)」、「高LDLコレステロール(4.5%)」であることを特定。これらを含む14の要因を一律に10%低減させるだけで、将来的に20万人以上の発症を抑制できる可能性が示されました。本研究成果は、2026年1月12日8:30(日本時間)に国際的医学誌「The Lancet Regional Health - Western Pacific」へ掲載されました。
<ポイント>
- 日本の認知症の約9%は、理論的に予防可能であることが、日本の公的データを用いた解析から明らかになった。
- 特に影響が大きい危険因子は、難聴、運動不足、高LDLコレステロールで、いずれも対策によって改善が期待できる。
- 危険因子を一律に10%低減できた場合、将来的に約20万人以上の認知症を予防できる可能性が示された。
- 本成果は、今後の認知症予防政策や健康施策の立案に活用できる科学的根拠として期待される。
■研究の背景
認知症は世界的に急増している深刻な公衆衛生課題です。認知症に伴う世界の経済的負担は、2019年時点で約1.3兆米ドルと推計されており、2030年には1.7兆米ドル、介護費用を含めると最大2.8兆米ドルにまで増加すると予測されています。
日本は世界で最も平均寿命が長く、急速に高齢化が進む「超高齢社会」です。65歳以上人口の割合は、2010年には21%を超え、2024年には29.3%に達しました。さらに2045年には、3人に1人以上が65歳以上になると見込まれています。加齢は認知症の最大の危険因子であることから、日本は世界でも特に認知症の影響を受けやすい国の一つと言えます。
厚生労働省の推計によると、2022年時点で65歳以上の約12.3%が認知症、約15.5%が軽度認知障害(MCI)とされています。認知症患者数は約443万人、MCIを含めると約1000万人にのぼり、2050年には認知症が約587万人(高齢者の15.1%)、MCIが約631万人(16.2%)に達すると予測されています。
近年、アミロイドβを標的とした抗体医薬など、新たな治療法が登場していますが、その効果や、高額な医療費や適応条件の厳しさなどから、実臨床での普及には課題が残っています。このため、「治療」だけでなく、発症そのものを遅らせる、あるいは防ぐ「予防」の重要性が増しています。
こうした流れの中で、権威ある医学誌「The Lancet」の認知症委員会(The Lancet Commission on dementia)は、生活習慣や環境要因などの介入可能な危険因子への対策により、世界全体で認知症の約45%が予防可能であると報告しています。しかし、これらの推計は主に欧米を中心とした国際データに基づくものであり、日本の社会構造や健康特性を十分に反映しているとは言えません。
そこで本研究では、日本の公的統計や疫学研究データを用いて、日本における認知症予防の潜在的可能性を定量的に評価しました。これは、今後増加が確実視される認知症に対し、どの危険因子に、どの程度、優先的に介入すべきかを示す科学的根拠を提供することを目的としています。
■研究の方法
本研究では、2024年のランセット認知症委員会の報告において、科学的根拠に基づき特定された以下の14の修正可能な認知症危険因子を対象に解析を行いました。
①教育歴の低さ、②難聴、③高LDLコレステロール血症、④うつ、⑤外傷性脳損傷、
⑥運動不足、⑦喫煙、⑧糖尿病、⑨高血圧、⑩肥満、⑪過剰な飲酒、⑫社会的孤立、
⑬大気汚染への曝露、⑭視力低下
これらの因子について、日本の国民健康・栄養調査、政府統計、疫学研究、環境データなど、信頼性の高い国内データを用いて、それぞれの有病率(該当者の割合)を推定しました。さらに、集団寄与危険割合(PAF)*1および潜在的影響割合(PIF)*2を算出し、日本における認知症予防の潜在的規模を定量的に評価しました。
■主な結果
各危険因子のPAFについて
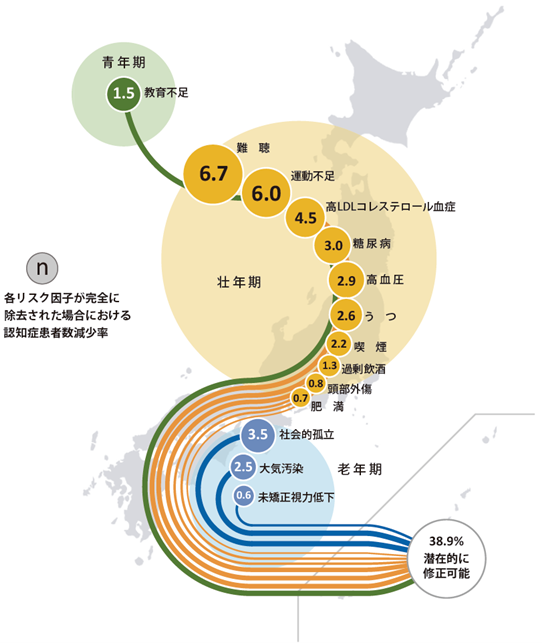
14因子すべてを考慮した場合、認知症の38.9%が予防可能であることが示されました。特に影響が大きい危険因子は、難聴(6.7%)、運動不足(6.0%)、高LDLコレステロール(4.5%)となっています。
各危険因子のPIFについて
・危険因子を一律に10%低減した場合、将来的に約20.8万人の認知症を予防
・危険因子を一律に20%低減した場合、将来的に約40.8万人の認知症を予防
|
【図】日本国内データを用いて算出した認知症発症に関連する14個の危険因子に関する寄与割合 Wasano K, Jørgensen K. The potential for dementia prevention in Japan: a population attributable fraction calculation for 14 modifiable risk factors and estimates of the impact of risk factor reductions. The Lancet Regional Health - Western Pacific 2026のSupplementより引用 |
※各因子が属する年代の分類について
図における各因子の青年期、壮年期、老年期という分類は、その時期に限定されるリスクであることを示すのではなく、「その時期以降」のリスクであることを示します。例えば最も大きな寄与度を示す難聴については、「55歳以上」と規定されていることから、壮年期に限らず老年期においても対策を行うことが重要です。
■本研究の意義
本研究は、日本の実情に即したデータを用いて、どの危険因子に優先的に介入すべきかを定量的に示した点に大きな意義があります。特に、難聴や運動不足など、適切な対策によって改善可能な要因が、認知症予防に大きく寄与することが明らかになりました。また、駐日デンマーク大使館ならびにヘルスケアデンマークの連携支援のもとで実施された日本とデンマークの学術連携による認知症研究の成果です。
本成果は、2024年に施行された認知症基本法や、今後の認知症施策の具体化に向けた科学的根拠として活用されることが期待されます。
本研究は、国立研究開発法人 日本医療研究開発機構(AMED) 障害者対策総合研究開発事業(身体・知的・感覚器障害分野)の支援を受けて実施しました。
■論文情報
◇掲載誌:The Lancet Regional Health - Western Pacific
◇公開日時:2026年1月12日8:30(日本時間)
◇論文タイトル:The potential for dementia prevention in Japan: a population attributable fraction calculation for 14 modifiable risk factors and estimates of the impact of risk factor reductions(日本における認知症予防の可能性:14個のリスク因子の集団寄与危険割合とリスク低減による効果の予測)
◇著者:和佐野浩一郎1, Kasper Jørgensen 2
1.東海大学医学部耳鼻咽喉科・頭頸部外科
2.コペンハーゲン大学認知症センター(Department of Neurology, Danish Dementia Research Centre, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark )
◇DOI:https://doi.org/10.1016/j.lanwpc.2025.101792
【用語説明】
*1 集団寄与危険割合(PAF:Population Attributable Fraction)
「もし特定の危険因子が存在しなかったと仮定した場合、全体の認知症のうち、どの程度が防げた可能性があるか」を示す指標。例えば、PAFが10%であれば、「理論的には、その因子がなければ認知症の10%は起こらなかった可能性がある」ことを意味します。本研究では、14因子それぞれのPAFを算出し、さらに因子同士の重なりを考慮した上で、全体としてどの程度の認知症が予防可能かを評価しました。
*2 潜在的影響割合(PIF:Potential Impact Fraction)
「危険因子を完全になくすのではなく、例えば10%や20%といった現実的な範囲で減らした場合に、どの程度の認知症が減少する可能性があるか」を示す指標。PAFが「理論上の最大限の予防可能性」を示すのに対し、PIFは実際の政策や介入によって達成し得る効果を見積もるための指標です。本研究では、14の危険因子をそれぞれ10%または20%低減した場合に、将来的にどれだけの認知症患者数を減らせる可能性があるかを推定しました。
|
<研究に関するお問い合わせ> 東海大学医学部耳鼻咽喉科・頭頸部外科 教授 和佐野浩一郎 TEL:0463-93-1121
<本件に関するお問い合わせ> デンマーク大使館 上席商務担当官 吉元美帆 TEL:03-3780 8735 東海大学医学部付属病院 事務部事務課(広報) TEL:0463-90-2001(直通) |
Potential for Dementia Prevention in Japan
- Nearly 40% of Dementia Cases Are Preventable -
~Hearing Loss Identified as the Leading Risk Factor, Followed by Physical Inactivity~
An international collaborative research group led by Professor Koichiro Wasano, MD, PhD. of the School of Medicine, Tokai University (Isehara Campus), together with Kasper Jørgensen, MSc, from the University of Copenhagen Dementia Research Centre (Denmark), has demonstrated that 38.9% of dementia cases in Japan are theoretically preventable through improvements in lifestyle and health-related factors.
This conclusion was drawn from analyses based on Japanese public statistics and epidemiological data.
The study identified hearing loss (6.7%) as the largest modifiable risk factor for dementia in Japan, followed by physical inactivity (6.0%) and high LDL cholesterol (4.5%). The findings further suggest that a uniform 10% reduction in these 14 modifiable risk factors could potentially prevent more than 200,000 future dementia cases nationwide.
These results were published on January 11, 2026, in the international medical journal The Lancet Regional Health - Western Pacific.
Key Points
- Analysis based on Japanese public and epidemiological data revealed that approximately 38.9% of dementia cases in Japan are theoretically preventable.
- The most influential modifiable risk factors were identified as hearing loss, physical inactivity, and high LDL cholesterol, all of which are amenable to preventive interventions.
- The findings suggest that a uniform 10% reduction in these risk factors could potentially prevent more than 200,000 future cases of dementia in Japan.
- These results are expected to serve as important scientific evidence to inform future dementia prevention policies and public health strategies.
Background
Dementia is a rapidly growing global public health challenge. The worldwide economic burden associated with dementia was estimated at approximately USD 1.3 trillion in 2019 and is projected to increase to USD 1.7 trillion by 2030, potentially reaching USD 2.8 trillion when including informal caregiving costs.
Japan has the longest life expectancy in the world and is experiencing rapid population aging, making it a so-called "super-aged society." The proportion of individuals aged 65 years and older exceeded 21% in 2010 and reached 29.3% in 2024. It is projected that by 2045, more than one in three people in Japan will be aged 65 years or older. Given that aging is the strongest risk factor for dementia, Japan is among the countries most vulnerable to the growing impact of dementia.
According to estimates from the Ministry of Health, Labour and Welfare, as of 2022, approximately 12.3% of adults aged 65 years and older had dementia, while 15.5% had mild cognitive impairment (MCI). This corresponds to approximately 4.43 million individuals with dementia, and nearly 10 million people when MCI is included. By 2050, the number of people with dementia is projected to reach 5.87 million (15.1% of the older population), with 6.31 million (16.2%) having MCI.
In recent years, novel disease-modifying therapies, including amyloid beta targeting monoclonal antibodies, have emerged. However, their real-world implementation remains limited due to modest clinical benefits, high costs, and strict eligibility criteria. As a result, increasing attention has been directed toward prevention, with the goal of delaying onset or reducing the incidence of dementia.
In this context, the Lancet Commission on Dementia has reported that up to 45% of dementia cases worldwide may be preventable through interventions targeting modifiable lifestyle and environmental risk factors. However, these estimates are largely based on data from Western countries and may not adequately reflect the social structure, health characteristics, and risk factor distribution specific to Japan.
Therefore, the present study aimed to quantitatively assess the potential for dementia prevention in Japan using Japanese public statistics and epidemiological data. The objective was to provide scientific evidence to identify which risk factors should be prioritized and to what extent, in order to effectively address the expected increase in dementia cases.
Methods
This study analyzed 14 modifiable risk factors for dementia identified in the 2024 Lancet Commission on Dementia, based on robust scientific evidence:
- Lower education
- Hearing loss
- High LDL cholesterol
- Depression
- Traumatic brain injury
- Physical inactivity
- Smoking
- Diabetes
- Hypertension
- Obesity
- Excessive alcohol consumption
- Social isolation
- Air pollution
- Untreated visual loss
For each risk factor, prevalence estimates were derived from reliable Japanese data sources, including the National Health and Nutrition Survey, government statistics, epidemiological studies, and environmental datasets.
Using these data, we calculated the Population Attributable Fraction (PAF) and the Potential Impact Fraction (PIF) to quantitatively evaluate the potential scale of dementia prevention in Japan.
Key Results
Population Attributable Fraction (PAF) *1
When all 14 risk factors were considered together, 38.9% of dementia cases in Japan were estimated to be preventable. The most influential risk factors were:
- Hearing loss: 6.7%
- Physical inactivity: 6.0%
- High LDL cholesterol: 4.5%
Potential Impact Fraction (PIF) *2
- A uniform 10% reduction in all modifiable risk factors could potentially prevent approximately 208,000 future cases of dementia.
- A uniform 20% reduction could potentially prevent approximately 408,000 future cases of dementia.
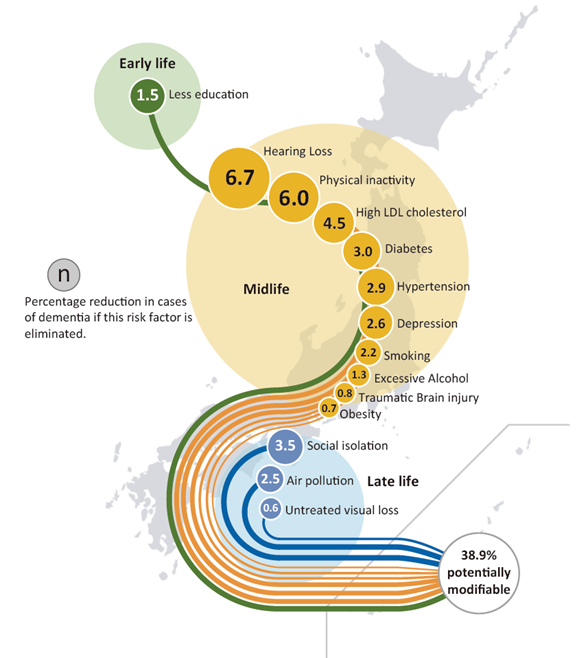
Figure Population attributable fraction (PAF) of potentially modifiable risk factors for dementia in Japan
●Note on the Classification of Life Stages for Each Risk Factor
In the figure, the classification of each risk factor into young adulthood, midlife, or late life does not indicate that the risk is confined to that specific life stage. Rather, it signifies that the risk emerges at that stage and persists thereafter. For example, hearing loss, which showed the largest contribution to dementia risk, is defined as affecting individuals aged 55 years and older. This indicates that preventive and intervention measures are important not only during midlife but also throughout later life.
■Significance of the Study
This study is significant in that it quantitatively identifies priority targets for intervention using data that accurately reflect the Japanese population and social context. In particular, the findings demonstrate that modifiable factors, such as hearing loss and physical inactivity, can make a substantial contribution to dementia prevention when appropriately addressed.
The study was conducted with the support of the Royal Danish Embassy, Japan, and Healthcare Denmark, which supported the collaboration through facilitation, convening and international outreach, and represents the fruit of academic collaboration between Japan and Denmark in the field of dementia research.
These findings are expected to serve as important scientific evidence for the implementation of the Basic Act on Dementia, which came into force in 2024, as well as for the development and refinement of future national dementia prevention strategies in Japan.
■Article information
◇Journal: The Lancet Regional Health - Western Pacific
◇Date of publishment: January 11 2026, 23:30 UTC/GMT
◇Title: The potential for dementia prevention in Japan: a population attributable fraction calculation for 14 modifiable risk factors and estimates of the impact of risk factor reductions
◇Author: Koichiro Wasano, MD, PhD 1, Kasper Jørgensen, MSc 2
1.Department of Otolaryngology, Head and Neck Surgery, Tokai University School of Medicine, Isehara, Japan
- Department of Neurology, Danish Dementia Research Centre, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
◇DOI:https://doi.org/10.1016/j.lanwpc.2025.101792
Glossary
*1 Population Attributable Fraction (PAF)
The Population Attributable Fraction (PAF) is an index that estimates the proportion of dementia cases that could theoretically have been prevented if a specific risk factor had been completely absent. For example, a PAF of 10% indicates that, in theory, 10% of dementia cases might not have occurred if that risk factor had not existed.
In this study, the PAF was calculated for each of the 14 modifiable risk factors. In addition, overlaps and interrelationships among the factors were taken into account to estimate the overall proportion of dementia that could potentially be prevented in the population.
*2 Potential Impact Fraction (PIF)
The Potential Impact Fraction (PIF) estimates the reduction in dementia incidence that could be achieved by realistically lowering the prevalence of risk factors, such as by 10% or 20%, rather than completely eliminating them.
While PAF represents the theoretical maximum preventable proportion, PIF provides a more practical estimate of the impact that actual public health policies and interventions could achieve. In this study, we estimated the potential reduction in the number of future dementia cases if each of the 14 risk factors were reduced by 10% or 20%, respectively.
|
<For Research Inquiries> Koichiro Wasano, MD, PhD Professor and Chairperson, Department of Otolaryngology and Head and Neck Surgery, Tokai University School of Medicine TEL:+81-(0)463-93-1121
<Public Relations Contact> Miho Yoshimoto Senior Commercial Officer Royal Danish Embassy, Tokyo, Japan TEL:+81 (0) 3-3780 8735
Tokai University Hospital Administration Division (Public Relations) TEL:+81- (0)463-90-2001(direct line) |